
We carried out a pilot, unblinded, 2-armed, parallel group, randomised managed trial of ‘Diabetes misery e-learning: A course for diabetes educators’ (Figs. 1 and a couple of). In June 2019 we commenced selling the research to CDEs in our present database who had expressed curiosity in analysis participation alternatives, and through well being skilled conferences/conferences and related skilled organisations. The promotional supplies directed potential contributors to a web site for self-registration of curiosity to take part within the research. The possible contributors have been screened for eligibility through a brief on-line Qualtrics survey. The eligibility standards have been: 1) certified and at present working as a CDE in Australia for ≥ 1 12 months, 2) direct involvement within the medical care of ≥ 10 adults with kind 1 or kind 2 diabetes per week, and three) desktop or laptop computer pc entry with an web connection.
Fig. 1
Examine design flowchart with participation and knowledge return abstract
Fig. 2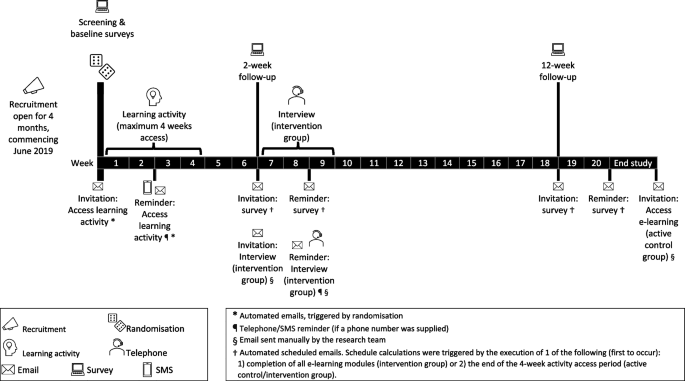
Timeline of the randomised managed trial
Following on-line completion of baseline survey questions (see Measures), eligible contributors have been randomly allotted (automated computer-generated, 1:1 ratio) to the intervention group (diabetes misery e-learning) or energetic management group (diabetes misery chapter). The pc-generated randomization was facilitated independently by the platform developer. Contributors have been instructed the way to entry their allotted studying exercise on the finish of the survey and through e-mail and had 4 weeks to entry the exercise.
At 2- and 12-weeks follow-up, all contributors have been invited to finish on-line (Qualtrics) surveys to evaluate instant and longer-term outcomes (e.g., implementation), respectively. To minimise lacking knowledge, all fastened alternative survey questions (in any respect timepoints) have been set as ‘pressured response’. The intervention group additionally supplied suggestions about acceptability and implementation of the e-learning of their 2-week follow-up survey and through a semi-structured phone interview. The interview strategies and findings shall be reported elsewhere.
Contributors finishing the research have been eligible to obtain a certificates, which might be used for skilled credentialling functions, and a tough copy of ‘Diabetes and Emotional Well being’. Interview contributors have been supplied entry to a prize draw ($200 voucher). No incentives have been supplied for survey return. The energetic management group have been supplied equal (4 weeks) entry to the e-learning on the finish of the research.
Studying actions
Energetic management contributors have been emailed a hyperlink to the diabetes misery chapter of ‘Diabetes and Emotional Well being’ [1, 22] and instructed to learn it. The chapter follows a 7As mannequin (AWARE, ASK, ASSESS, ADVISE, ASSIST, ASSIGN, and ARRANGE) to information learners in a stepwise course of for figuring out and addressing diabetes misery. The chapter was developed in session with stakeholders and has foundations in person-centred care [22]. It gives complete evidence-based details about diabetes misery, together with indicators to search for, recommended open-ended questions, and case research. It additionally features a copy of the Drawback Areas in Diabetes scale (PAID; a validated diabetes misery questionnaire) with steerage about scoring, interpretation, and dialogue. It’s freely obtainable on-line (www.ndss.com.au). A abstract of the chapter content material is supplied in Complement 1.
Intervention contributors have been emailed a hyperlink to the e-learning and instructed to entry it. The e-learning comprises comparable data to the diabetes misery chapter. The important thing distinction is that the e-learning is interactive, with better emphasis on abilities improvement, knowledgeable by academic and behavioural theoretical fashions. For instance, it contains studying aims, movies demonstrating session abilities, and actions (e.g., alternatives to verify understanding, observe abilities, self-reflect, and plan actions). It was developed utilizing intervention mapping, a complete best-practice framework for informing the planning, improvement and analysis of an intervention [26]. Extra particulars in regards to the platform, e-learning content material, and analysis plan (e.g. pre-defined research design and outcomes of curiosity) are revealed elsewhere [26].
Pattern dimension and ‘cease/go’ standards
Whereas pilot research don’t require a pattern dimension calculation, we aimed for N= 50, anticipating 20% attrition, permitting for at least 10 contributors per arm [27]. We monitored participant recruitment, engagement with the intervention (module completion) and follow-up knowledge return to make sure ample knowledge have been collected. No ‘cease/go’ standards (apart from achievement of pattern dimension) or interim analyses have been deliberate or carried out.
Deviations from protocol
The research promotion and recruitment interval was prolonged from 2 months, to about 4 months, as a result of slower than anticipated uptake and low follow-up survey response charges. We added reminders to take part, for each the training exercise and follow-up knowledge assortment. We prolonged the training exercise entry timeframe from 2 to 4 weeks for all contributors, following early participant suggestions that 2 weeks was too quick due given busy medical schedules. We recruited greater than the deliberate 50 contributors as a result of greater than anticipated attrition. As a result of lengthening of timeframes for recruitment and exercise entry, we accomplished knowledge assortment in early in 2020, which was later than initially deliberate.
Outcomes
Examine design feasibility: Recruitment pace/success, exclusion standards suitability (charges of and causes for exclusion), engagement (participant withdrawals and studying exercise entry), attrition (follow-up knowledge return), and suitability of study-specific measures (ground/ceiling results, scale reliability of the arrogance and significance survey measures).
Intervention acceptability: Intervention completion instances, variety of modules accessed, consumer scores of intervention high quality and acceptability (see Survey measures).
Preliminary proof of results: CDEs’ diabetes distress-related information, motivation, confidence, behavioural abilities, and obstacles to implementation (see Survey measures).
Survey measures
Knowledgeable by an intervention mapping course of (described elsewhere [26]), study-specific survey questions have been developed to measure intervention high quality and acceptability and preliminary proof of results:
-
High quality, acceptability, and future functions (2-week follow-up; intervention group solely): Twenty-six objects assessed consumer experiences together with the standard and relevance of the content material, suitability and ease-of-use of the platform, and future functions. Of those 25, have been assessed on a 4-point scale (’strongly disagree’ to ‘strongly agree’) and 1 query had a ‘sure/no’ response format. 4 further questions assessed the appropriateness of the time required, issue degree and technical issues.
-
Data (all timepoints; all contributors): Twelve questions on their information of diabetes misery (response choices: true/false/I don’t know). Every e-learning module was represented by 1–2 questions. Appropriate responses have been summed (potential scores: 0–12), with greater scores indicating better information of diabetes misery.
-
Perceived significance of offering help (all timepoints; all contributors): Three scales with objects describing medical behaviours/actions: establish diabetes misery (5 objects), help with diabetes misery (three objects), and refer for diabetes misery (three objects) (Complement 2). For every merchandise, contributors rated the significance of every motion on a 4-point scale (0 = ‘under no circumstances essential’ to three = ‘crucial’). For every of the three scales, the merchandise scores have been summed to kind a complete rating.
-
Confidence to supply help (all timepoints; all contributors): The identical scales/actions/scoring have been repeated because the ‘significance’ objects, however contributors have been requested to point their confidence to implement every motion (0 = ‘under no circumstances assured’ to three = ‘very assured’).
-
Behavioural abilities (all timepoints; all contributors): One query enquired in regards to the proportion of adults with kind 1 or kind 2 diabetes the CDE requested “how they really feel about residing with and managing diabetes” prior to now 2 weeks (i.e., Ask about diabetes misery). Two equally worded query enquired about evaluation of diabetes misery (i.e., the proportion they invited to finish a diabetes misery questionnaire, e.g., PAID or Diabetes Misery Scale) and evaluation of psychological well being (i.e., the proportion they invited to finish one other psychological questionnaire, e.g., Affected person Well being Questionnaire 9, Kessler Psychological Misery Scale 10, or World Well being Organisation Wellbeing Index 5). All objects have been rated on a 4-point scale (0 = ‘none of them’ to three = ‘all of them’).
-
Office and systemic obstacles (all timepoints; all contributors): Contributors rated the extent to which 18 potential obstacles/enablers have an effect on them in offering help for diabetes misery. The objects (e.g., office set-up and insurance policies, entry to instruments and sources, psychological well being referral choices, funding and remuneration) have been every rated on a 5-point scale (-2 = ‘hinders me rather a lot’ to 2 = ‘helps me rather a lot’).
As well as, at baseline, contributors accomplished eleven objects about their demographic {and professional} traits (e.g., age, gender, career, office geography and setting). Additionally they reported on related Prior related skilled improvement through 2 questions: whether or not they had beforehand: a) learn ‘Diabetes and Emotional Well being’ (response choices: sure—partially, sure – in full, no); b) participated (in previous 5 years) in session abilities coaching (response choices: sure/no). We listed varied coaching examples related to diabetes, psychological well being, communication, and counselling abilities (e.g., Dose Adjustment For Regular Consuming (DAFNE) or Diabetes Schooling and Self-Administration for Ongoing and Newly Recognized (DESMOND) facilitation, acceptance dedication remedy, motivational interviewing, psychological well being evaluation or counselling, session abilities masterclass) as prompts.
Evaluation
Descriptive statistics have been used to explain participant traits, e-learning acceptability, and obstacles to help. The inner consistency reliability of the significance and confidence scales was evaluated utilizing the baseline survey knowledge (Cronbach’s alpha, α > 0.7 was deemed acceptable). Preliminary impact of the e-learning program was explored by evaluating inside group adjustments over time utilizing Wilcoxon Signed Rank Checks and impact sizes (r values). Most analyses have been carried out in SPSS (28.0.0.0, 190). Wilcoxon Signed Rank Checks impact sizes have been calculated in Microsoft Excel (2203, 16.0.15028.20178). The e-learning time dedication was calculated in Microsoft Excel, knowledgeable by web site analytics.